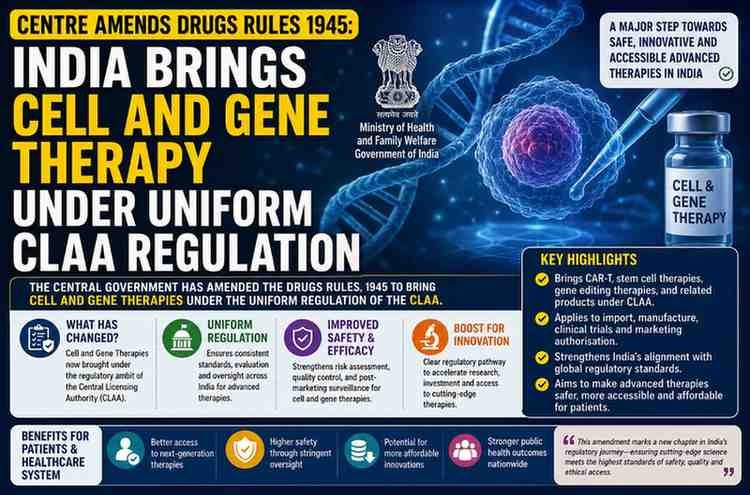
India’s cell and gene therapy sector just got aregulatory upgrade and it’s about time. On July 2, 2026, the Ministry ofHealth and Family Welfare announced that the Centre has amended theDrugs Rules, 1945, bringing cell or stemcell-derived products, gene therapeutic products, and xenografts under theCentrally License Approving Authority (CLAA)framework. The move, notified by the Ministry, is designed toclose a regulatory gap that has existed for years: while cutting-edgetreatments like CAR-T cell therapy raced ahead in Indian hospitals, therulebook governing them lagged behind, leaving licensing scattered andinconsistent across states.
In short who: the Central Government, through theMinistry of Health and Family Welfare and the Central Drugs Standard ControlOrganisation (CDSCO); what: an amendment to the Drugs Rules, 1945, expandingthe CLAA framework; when: notified in early July 2026; where: applicablenationwide across all Indian states; why: to standardise licensing andstrengthen patient safety oversight for advanced therapies; and how: by placingthese products under joint Central-State licensing authority, rather than leavingthem to fragmented state-level approval.
This isn’t just bureaucratic housekeeping. For acountry that wants to become a global hub for regenerative medicinemanufacturing, this amendment is a foundational move and it carries realimplications for patients, biotech startups, hospitals, and investorsalike.
What Exactly Changed in the Drugs Rules,1945?
Until this amendment, the CLAA framework themechanism under which the Centre and states jointly regulate certain high-riskdrug categories — covered a defined list of products: vaccines, large-volumeparenterals (IV solutions above 100 ml), and recombinant DNA-derived medicines.Advanced cell and gene therapies were conspicuously missing from that list, evenas they moved from experimental labs into mainstream cancer wards.
The new notification adds three categories to theCLAA umbrella:
- Cell or Stem Cell-derivedproducts including regenerative treatments and CAR-T celltherapies used against blood cancers such as leukemia and lymphoma
- Gene therapeuticproducts covering gene replacement and gene-editing treatmentsused for genetic disorders and several cancer types
- Xenografts animaltissue-derived products, such as heart valves, used in cardiology andorthopedic transplants
The government’s stated rationale isstraightforward: these are “highly complex, specialised and rapidlyevolving areas of medical science” that demand a higher degree of scrutinythan conventional pharmaceuticals. By folding them into CLAA, manufacturers andclinics offering these therapies will now need central approval alongsidestate-level licensing a dual-check system intended to prevent the kind ofregulatory arbitrage that can occur when standards differ from state tostate.
Why This Matters: The Regulatory Gap India JustClosed
To understand why this amendment matters, it helpsto look at what was happening on the ground before it. India’s drug licensingsystem has traditionally operated on a split model some products fallentirely under state licensing authorities, while a smaller, higher-riskcategory falls under the CLAA’s joint Central-State oversight. Advanced celland gene therapies had, until now, effectively slipped through this gap. A stemcell clinic in one state could operate under a different approval standard thana similar clinic in another state, creating inconsistency in safety protocols,quality benchmarks, and accountability.
This patchwork approach became increasingly riskyas demand for these treatments surged. Unregulated or loosely regulated stemcell clinics have been a known problem in India for years, with reports ofpatients receiving unproven “stem cell therapies” for conditionsranging from autism to spinal injuries treatments with little clinicalevidence behind them and minimal oversight of how the cells were sourced,processed, or administered. By centralising licensing for this category, thegovernment is effectively raising the entry barrier for anyone offering thesetherapies, which should, in theory, squeeze out operators who were cuttingcorners.
A Quick Timeline: How We Got Here
| Period | Development |
|---|---|
| Pre-2020s | Cell and gene therapies largely absent frommainstream Indian clinical practice; regulation limited andinconsistent |
| Early-to-mid 2020s | CAR-T cell therapies (including India’s firstindigenously developed CAR-T product) enter clinical use for blood cancers;stem cell-based treatments proliferate across private clinics |
| 2025 | Ministry of Health circulates draft amendments toDrugs Rules for stakeholder consultation, alongside other CDSCO regulatoryupdates |
| July 2026 | Centre formally notifies amendment bringingcell/stem cell products, gene therapeutics, and xenografts under the CLAAframework |
How the CLAA Framework Actually Works
For readers unfamiliar with Indian drug regulation,the CLAA framework is essentially India’s answer to the question: whichproducts are too high-risk to be regulated by a single state alone? Under thissystem, manufacturing and marketing licenses for CLAA-listed products requiresign-off from the Central Licensing Authority (via CDSCO) in addition to therelevant State Licensing Authority. This joint structure is meant to combinelocal implementation capacity with centralised technical expertise — the statehandles ground-level inspection and enforcement, while the Centre sets andmonitors the scientific and safety benchmarks.Recombinant DNA-based medicines were added to this list someyears ago precisely because biotechnology products carry manufacturing andsafety complexities that traditional chemical drugs don’t. Cell and genetherapies are, in many ways, even more complex living cells engineeredoutside the body, reintroduced into a patient, with manufacturing processesthat can vary batch to batch. That complexity is exactly why regulatorsworldwide, including the US FDA’s Center for Biologics Evaluation and Researchand the UK’s MHRA, treat these products as a distinct regulatory categoryrequiring specialised evaluation pathways rather than forcing them throughgeneric drug-approval processes.
The Bigger Picture: India’s Bid to Be a Global CGTHub
This is where the story gets more interesting thana routine regulatory notification. India has ambitions to become a seriousplayer in the global cell and gene therapy (CGT) manufacturing landscape — notjust as a consumer of these expensive, often imported treatments, but as aproducer and exporter. The country already has a track record in genericpharmaceuticals and biosimilars; the next frontier is advancedtherapeutics.
But investors, especially international ones, lookclosely at regulatory clarity before committing capital to a market. Afragmented, state-by-state approval system for something as sensitive asgene-editing products is a red flag for any multinational biotech consideringIndia as a manufacturing base. By aligning cell and gene therapy oversight witha unified national framework, the Centre is signalling to global biotechcompanies — and to Indian firms with export ambitions that the country isserious about matching international regulatory rigour.
This is a strategic parallel worth drawing out:just as India’s push toward BIS and ISO harmonisation helped its manufacturingexports gain global trust, aligning CGT regulation with frameworks resemblingthe FDA and EMA’s advanced therapy medicinal product (ATMP) pathways could helpIndian-made cell and gene therapies gain easier acceptance in export markets.It’s not a cosmetic change it’s a trust-building exercise aimed at globalmarkets.
Real-World Impact: What Changes for Patients,Hospitals, and Startups
It’s worth being precise about what this amendmentdoes and doesn’t do. It does not immediately change patient access totreatment, alter drug pricing, or approve any new therapy. What it changes isthe regulatory pathway products must pass through before reaching patients.Here’s how different stakeholders are likely to feel the effects:
- Patients: Over time,expect greater consistency in safety standards regardless of which state atreatment is administered in. This should, in principle, reduce the risk ofunproven or poorly manufactured cell therapies being marketed to vulnerablepatients a long-standing concern in India’s semi-regulated stem cell clinicindustry.
- Hospitals and treatmentcentres: Facilities offering CAR-T therapy, stem celltreatments, or xenograft procedures will now need to navigate central licensingrequirements in addition to existing state approvals, likely lengtheninginitial compliance timelines but improving long-term credibility.
- Biotech startups andmanufacturers: Smaller Indian biotech firms developing cell andgene therapy products may face higher upfront compliance costs and morerigorous documentation requirements. This could be a genuine challenge forearly-stage companies without deep regulatory-affairs resources, even as itbenefits the sector’s overall credibility.
- Investors: A unifiednational framework reduces regulatory uncertainty historically one of thebiggest deterrents to biotech investment in emerging markets.
What Competitors’ Coverage Is Missing
Most coverage of this amendment has stopped atreporting the notification itself. Few outlets have pointed out an importantnuance: centralising licensing tends to raise compliance costs before itimproves access. Historically, when India has tightened CLAA-style oversightfor other product categories, there has been a short-term slowdown in newlicenses as companies adjust to stricter documentation and inspectionrequirements, followed by longer-term gains in quality and market confidence.Expect a similar pattern here a period of adjustment for existing stem celland cell-therapy operators over the next 12 to 18 months, followed by a moreconsolidated, credible industry.
There’s also an enforcement question that deservesmore scrutiny than it’s getting. India has no shortage of well-designed ruleson paper; the persistent challenge has been inspection capacity andfollow-through at the state level. Unless CDSCO and state drug authorities areresourced to actually audit cell and gene therapy manufacturing facilities —which require specialised technical expertise to inspect properly, unlikeconventional drug plants this amendment risks becoming a compliance formalityrather than a genuine safety upgrade. That’s the detail worth watching in thecoming months: whether the government pairs this rule change with investment ininspector training and lab infrastructure.
Conclusion: A Necessary Step, With the Real TestStill Ahead
The amendment to the Drugs Rules, 1945 is asensible and overdue correction to a regulatory blind spot in India’shealthcare framework. Bringing cell or stem cell-derived products, genetherapeutic products, and xenografts under the CLAA umbrella brings India’soversight of advanced therapies closer to the standards followed by regulatorslike the FDA and MHRA, and it addresses a genuine patient-safety problemcreated by inconsistent state-level rules.But regulatory text is only as good as its enforcement. Thereal measure of this amendment’s success won’t be the notification itself itwill be visible over the next few years in whether India’s cell and genetherapy sector sees fewer reports of unregulated stem cell clinics, faster andmore predictable approval timelines for legitimate CAR-T and gene therapyproducts, and growing confidence from global biotech investors eyeing India asa manufacturing base. If the Centre backs this rule change with adequateinspection capacity and clear implementation guidelines, it could mark agenuine turning point for one of the most promising and previouslyunder-regulated corners of Indian medicine.
For breaking news and live news updates, like us on Facebook or follow us on Twitter and Instagram. Read more on Latest Health on thefoxdaily.com.



COMMENTS 0