Multiple sclerosis is a chronic, immune-mediated disease of the central nervous system in which the body’s own immune cells attack myelin the protective sheath surrounding nerve fibres in the brain and spinal cord. As myelin is damaged and, in progressive cases, the underlying nerve fibres themselves are compromised, the transmission of electrical signals between the brain and the rest of the body becomes disrupted, slowed, or entirely blocked. The result is a constellation of neurological symptoms whose variety and unpredictability make MS one of the most diagnostically challenging conditions in modern medicine.
What makes early detection particularly difficult is that MS does not announce itself with a single, unmistakable symptom. Its earliest manifestations are frequently diffuse, intermittent, and easily attributed to more common explanations stress, overwork, vitamin deficiency, or simply ageing. A person experiencing their first episode of MS-related fatigue is far more likely to assume they need more sleep than to consult a neurologist. This gap between symptom onset and diagnosis, which in some patients extends to years, represents the window where early intervention could most meaningfully alter the disease’s trajectory.
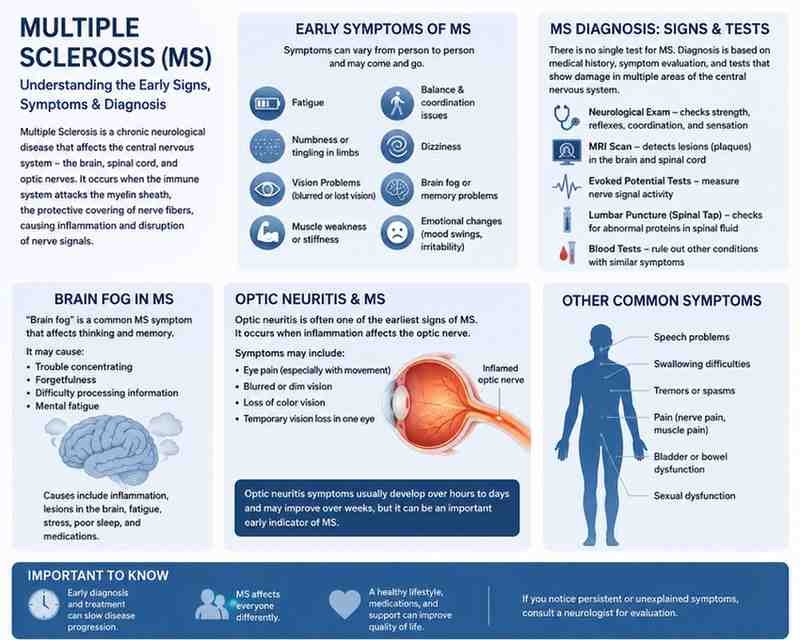
Fatigue: The Most Prevalent and Most Misunderstood Early Sign
Neurologists consistently identify fatigue as the single most common early symptom of multiple sclerosis, affecting approximately 80 percent of MS patients at some point in their disease course and frequently appearing before a formal diagnosis is established. What distinguishes MS-related fatigue from ordinary tiredness is not merely its severity but its character: it is disproportionate to activity level, not reliably resolved by rest, and often worsened by heat a phenomenon known as Uhthoff’s phenomenon, which occurs because elevated body temperature further impairs conduction in already-compromised nerve fibres.
Patients describing early MS fatigue frequently struggle to communicate its quality to physicians accustomed to evaluating fatigue in the context of anaemia, thyroid dysfunction, or depression. The experience is often described as a profound neurological heaviness a sense that the body’s energy reserves have simply been withdrawn without explanation, independent of how much sleep was obtained the previous night. This lassitude can fluctuate dramatically across the day, often worsening in the afternoon and improving after brief rest, a pattern that neurologists flag as clinically suggestive when combined with other early indicators.
Weakness and Coordination Problems: When the Body Stops Responding Reliably
Limb weakness, most commonly affecting one side of the body or a single limb in the early stages, represents another frequently reported early symptom of MS. Unlike the generalised weakness associated with systemic illness, MS-related weakness tends to be focal concentrated in a specific muscle group and may be accompanied by spasticity, a stiffening or tightening of muscles that creates resistance to movement. Patients often describe their leg as feeling unusually heavy when climbing stairs, or notice an unexplained tendency to trip over minor obstacles on even surfaces.
Balance and coordination difficulties formally referred to as cerebellar or proprioceptive dysfunction frequently accompany weakness in early MS presentations. Difficulty maintaining balance when standing with eyes closed, a subtle deterioration in fine motor tasks such as writing or buttoning clothing, or an unsteady gait that appears to worsen when the person is tired all represent clinical warning signs that warrant neurological assessment. These symptoms reflect demyelination in the cerebellum or its connecting pathways, regions of the central nervous system particularly vulnerable in early MS.
Brain Fog: The Cognitive Dimension That Diagnosis Often Overlooks
Cognitive symptoms in multiple sclerosis have historically been underrecognised in clinical assessments focused primarily on motor and sensory deficits, but neurological research over the past two decades has established their early presence as both common and functionally significant. The experience patients typically describe as brain fog encompasses a cluster of specific cognitive impairments: slowed information processing speed, difficulty with working memory, reduced ability to sustain attention, and word-finding problems that are distinct from the broader language difficulties associated with stroke or dementia.
The practical consequences of MS-related cognitive dysfunction in the early stages are often more disruptive to daily functioning than the motor symptoms that more readily attract clinical attention. A professional who finds themselves taking three times as long to complete a familiar task, repeatedly losing the thread of a meeting, or struggling to recall words they have used fluently for decades may be experiencing early demyelination in the cognitive networks of the cerebral cortex even in the absence of any physical symptoms that would conventionally prompt neurological referral.
Visual Disturbances: The Symptom Most Likely to Trigger Timely Diagnosis
Optic neuritis inflammation of the optic nerve is among the most clinically recognisable early presentations of multiple sclerosis and, crucially, among the most likely to prompt the kind of urgent specialist referral that enables timely diagnosis. It typically presents as a unilateral reduction in visual acuity, pain with eye movement, and a loss of colour saturation colours appearing washed out or desaturated in the affected eye that develops over hours to days.
Approximately 20 to 30 percent of MS patients experience optic neuritis as their presenting symptom, and in a significant proportion of cases, a first episode of optic neuritis in a young adult is the event that ultimately leads to an MS diagnosis following MRI investigation. Double vision (diplopia), caused by lesions affecting the nerves controlling eye movement, represents a related but distinct early visual symptom that neurologists consider equally suggestive of demyelinating disease when it occurs in the appropriate clinical context.
Sensory Symptoms: Pins, Needles and the Invisible Neurological Warning
Abnormal sensations paraesthesias are among the earliest and most frequently reported symptoms in MS, yet their very ordinariness means they are routinely dismissed by patients and, occasionally, by non-specialist clinicians. Tingling, numbness, a sensation of tight banding around the torso or limbs, or the feeling that a limb has fallen asleep without the usual postural explanation all reflect early demyelination in sensory pathways of the spinal cord or brain.
A particularly diagnostically significant sensory phenomenon is Lhermitte’s sign an electric shock-like sensation that travels down the spine and into the limbs when the neck is flexed forward. While not exclusive to MS, its presence in a young adult with other suggestive symptoms is considered a strong clinical indicator of cervical spinal cord demyelination and warrants prompt MRI investigation. Patients experiencing this phenomenon frequently describe it as startling and unmistakable, though they may not spontaneously volunteer it unless specifically asked.
| Early Symptom | Clinical Description | Prevalence in MS | Common Misdiagnosis | When to Seek Neurology Review |
|---|---|---|---|---|
| Fatigue | Disproportionate, heat-sensitive, not resolved by rest | ~80% | Depression, anaemia, thyroid disorder | Persistent >6 weeks, unrelated to activity |
| Limb Weakness | Focal, asymmetric, may include spasticity | ~40–50% | Orthopaedic injury, vitamin B12 deficiency | Progressive or recurrent episodes |
| Brain Fog | Slowed processing, word-finding difficulty, memory lapses | ~50–65% | Anxiety, burnout, sleep disorder | Interfering with work or daily function |
| Optic Neuritis | Unilateral vision loss, eye pain, colour desaturation | ~20–30% | Migraine aura, retinal issue | Immediately urgent ophthalmology and neurology |
| Sensory Disturbances | Tingling, numbness, Lhermitte’s sign | ~40–45% | Peripheral neuropathy, cervical spondylosis | Recurrent, migratory, or lasting >24 hours |
| Bladder Dysfunction | Urgency, frequency, incomplete emptying | ~33% early stage | UTI, overactive bladder | Recurrent UTI without infection confirmed |
Bladder and Bowel Symptoms: The Early Signs Nobody Discusses
Urinary urgency, increased frequency, difficulty initiating urination, or the sensation of incomplete bladder emptying affect a substantial proportion of MS patients and can appear early in the disease course yet they are among the least discussed early symptoms, partly because patients are often reluctant to raise them and partly because they overlap with multiple other common conditions. Recurrent urinary tract infections that are confirmed on culture and treated appropriately, only to recur without clear explanation, have in some cases been the indirect clinical trail that ultimately led to an MS diagnosis when a neurologist considered demyelination of the spinal cord pathways controlling bladder function.
Bowel symptoms primarily constipation, though urgency and incontinence can also occur similarly reflect disruption of the autonomic nervous system pathways that travel through the spinal cord and are therefore vulnerable to the same demyelinating process affecting other neurological functions. These symptoms warrant clinical attention not only as potential MS indicators but in their own right, given their significant impact on quality of life.
Who Is Most at Risk: Understanding MS Demographics in India
Multiple sclerosis was historically considered rare in South Asian populations, a perception that has been substantially revised by improved diagnostic capacity and increased clinical awareness over the past two decades. Indian neurological registries now document a meaningful and apparently growing burden of MS, with estimates suggesting a prevalence of between 7 and 30 cases per 100,000 population depending on the region and study methodology figures that, applied to India’s population, represent hundreds of thousands of affected individuals.
The demographic profile of MS in Indian patients shares key features with global patterns: onset most commonly occurs between the ages of 20 and 40, women are affected at approximately twice the rate of men, and urban populations show higher prevalence rates than rural ones a pattern that may reflect both diagnostic ascertainment bias and genuine environmental or lifestyle-related risk factor differences. A family history of MS modestly elevates risk, and low vitamin D status highly prevalent across Indian demographic groups has been associated with increased MS risk in multiple epidemiological studies, though causality remains under investigation.
The Diagnostic Journey: What Happens After Symptoms Prompt a Referral
When a constellation of early symptoms prompts neurological assessment, the diagnostic process for MS has been substantially standardised through the McDonald Criteria an internationally used framework that integrates clinical history, neurological examination, MRI findings, and in some cases cerebrospinal fluid analysis to establish a diagnosis based on evidence of demyelinating lesions disseminated in both space (affecting multiple locations in the central nervous system) and time (occurring at more than one point in time).
MRI of the brain and spinal cord with gadolinium contrast enhancement is the most informative single investigation in the diagnostic workup, capable of identifying characteristic lesion patterns periventricular, juxtacortical, infratentorial, and spinal cord lesions with high sensitivity. The importance of prompt MRI in patients presenting with a clinically isolated syndrome (a first neurological episode suggestive of demyelination) cannot be overstated: evidence of subclinical lesions on MRI at the time of a first clinical episode substantially predicts conversion to definite MS and can inform decisions about early disease-modifying therapy.
Why Early Diagnosis Changes Everything
The therapeutic landscape for multiple sclerosis has been transformed over the past three decades. Where neurologists once had limited options beyond managing acute relapses with corticosteroids, the current armamentarium of disease-modifying therapies ranging from injectable interferons and glatiramer acetate to highly efficacious oral and infusion-based agents offers genuine capacity to reduce relapse frequency, slow disability accumulation, and in some cases substantially alter the long-term disease course.
The critical qualifier is timing. Disease-modifying therapies are most effective when initiated early in the disease course, before cumulative inflammatory damage has produced irreversible neurological deficits. The transition from relapsing-remitting MS the most common early disease pattern, characterised by discrete episodes of neurological dysfunction followed by partial or complete recovery to secondary progressive MS, in which disability accumulates more steadily, is influenced in part by the adequacy of early treatment. Every year of delayed diagnosis is, in the current therapeutic environment, a year of potentially preventable inflammatory activity.
The neurologist’s guidance on early MS warning signs carries a message that extends beyond symptom checklists: that fatigue, brain fog, and sensory disturbances are not merely inconveniences to be managed with lifestyle adjustments, but potential clinical signals deserving the same investigative rigour as any other neurological symptom and that the patients most likely to benefit from this recognition are those who act on it earliest.
For breaking news and live news updates, like us on Facebook or follow us on Twitter and Instagram. Read more on Latest Lifestyle on thefoxdaily.com.



COMMENTS 0